
⏱ 4 min read, 4 min video
Delirium is a sudden, confused state of mind. Up to 3 out of 4 older people can experience delirium after surgery or a serious illness. It can happen in any setting, but is common for people to develop delirium in intensive care units, palliative care, or long-term care homes as well. Learn more about what can trigger delirium, the signs and symptoms, and who is most at risk in this short video.
View or download transcript.
Sebastian's story: A sudden change
When Mark went to visit his 76-year-old father, Sebastian, in the hospital, he expected to find him resting quietly after hip replacement surgery. Sebastian had been living with dementia for three years, but his condition was usually stable and predictable. However, the scene Mark encountered was deeply alarming.
The nursing staff informed Mark that Sebastian had not slept, had repeatedly tried to climb out of bed unsupervised, and had nearly fallen, necessitating the installation of a bed alarm. Inside the room, the bed was in total disarray. Sebastian spoke in hushed, paranoid tones, claiming he had seen an armed gunman in the hallway and heard people outside the room plotting against him. Convinced he "might be next," he insisted on leaving the hospital immediately.
This sudden, drastic shift in Sebastian’s mental state was not a natural progression of his dementia, nor was it "just a part of aging." It was a medical emergency known as delirium.
Defining delirium: A sudden shift
Delirium is a sudden, confused state of mind. Unlike chronic cognitive conditions such as dementia, it is a rapid change in attention, awareness, and thinking. It is not a disease itself, but rather a high-priority signal that the brain is reacting to an underlying medical condition, an infection, or the side effects of medications. It is important to understand that the "trigger" is often not a brain disease itself; for example, another condition such as a urinary tract infection or a lung issue can cause the brain to enter this state of confusion.
There are two critical characteristics of delirium that family members should note:
- Rapid onset: It usually develops over a very short period, typically hours or a few days.
- Fluctuation: Symptoms tend to vary throughout the day; a person may seem perfectly clear one hour and highly confused the next.
While delirium is frequently associated with hospital stays, it can occur in any setting, including long-term care homes or at home.
Delirium vs. dementia: Understanding the difference
Because both conditions involve confusion and memory issues, they are often mistaken for one another. However, they are distinct. It is also important to note that while they are different, having dementia significantly increases a person's risk of developing delirium.
Table 1: Comparing delirium and dementia
| Feature | Delirium | Dementia |
| Onset | Sudden (hours or days). | Slow (months or years). |
| Daily Pattern | Fluctuates; symptoms change during the day. | Stable; symptoms do not change dramatically day-to-day. |
| Duration | Usually temporary; clears up in days or weeks. | Usually permanent and progressive. |
Who is at risk and what to watch for
Delirium can happen to anyone, but certain factors increase vulnerability. Statistically, up to 3 out of 4 older adults may experience delirium following a major surgery or a serious illness.
Risk factors:
- Age 65 or older.
- Recent surgery (particularly hip or heart surgery).
- Current infections, such as a urinary tract infection (UTI) or pneumonia.
- Pre-existing memory or thinking problems (cognitive impairment).
- Poor eyesight or hearing.
- Dehydration or severe illness (e.g., heart failure or lung problems).
- Use of certain medications, including sedatives or strong pain relievers like opioids.
Common symptoms:
- Disturbed attention: Being easily distracted or unable to follow a conversation.
- Disorganized thinking: Saying things that are mixed up or do not make sense.
- Hallucinations and delusions: Seeing or hearing things that aren’t real, or having paranoid ideas that others are trying to cause harm.
- Changed activity levels: This can range from "hyperactive" (restlessness and agitation) to "hypoactive" (drowsiness, sluggishness, apathy, or being unusually withdrawn).
Note on the "quiet" danger: Hypoactive delirium is often missed because the person is quiet and not "causing trouble." However, this sluggish, withdrawn state is just as much a medical emergency as loud agitation and requires immediate attention.
How family members can help
Family members are often the first to notice the subtle fluctuations that signal delirium. Your involvement is crucial for both prevention and recovery. Here are six proven strategies for preventing delirium:
- Reorientation: Frequently remind your loved one of the current date, time, and where they are. If they are in the hospital, gently explain why they are there and provide reassurance.
- Mental and physical stimulation: Engage them in quiet conversation or read aloud. Help them stay as physically active as is safely possible to encourage a normal sleep-wake cycle.
- Track medications: Maintain a comprehensive list of all medications, including over-the-counter drugs and supplements, to share with the medical team.
- Optimize senses: Ensure they have their glasses and that their hearing aids are clean and being worn.
- Environmental support: Keep the area quiet at night to encourage sleep. Bring familiar items from home—such as a clock, a calendar, or favourite photos—to help them feel secure.
- Healthy eating and drinking: Dehydration is a major trigger for delirium. Encourage and help your loved one with regular intake of fluids and healthy foods.
Ask About the HELP Program: If your loved one is in the hospital, ask the staff if they have a Hospital Elder Life Program (HELP). This is a specialized team dedicated to preventing delirium in older adults.
A Note on Caregiver Well-Being: Witnessing a loved one in a state of delirium can be distressing. Remember that the person "is not themselves" and may say things they will not remember later. Take breaks, eat well, and seek support from the healthcare team.
Delirium is preventable
Delirium is a medical emergency. If you suspect a loved one is experiencing these symptoms—even if they are simply unusually "quiet" or withdrawn—contact a healthcare provider immediately or go to the nearest emergency department.
In Sebastian’s case, Mark acted quickly by informing the nursing staff that his father’s paranoid thoughts were uncharacteristic. The medical team immediately performed a physical exam, checked his vital signs, and ordered a chest X-ray and urine sample to rule out an underlying infection. When the tests came back negative, they determined the delirium was a reaction to his surgical anesthetic and pain medications.
By adjusting his medications and having the family help with reorientation, Sebastian began to improve. Mark’s family brought in his favourite foods to encourage him to eat and kept a bedside calendar to help him track the days. Sebastian’s confusion eventually cleared, and he made a full recovery.
A helpful resource
The infographic below, from the Regional Geriatric Program of Toronto, summarizes the 6 strategies to prevent delirium in older adults. Download a copy and share.
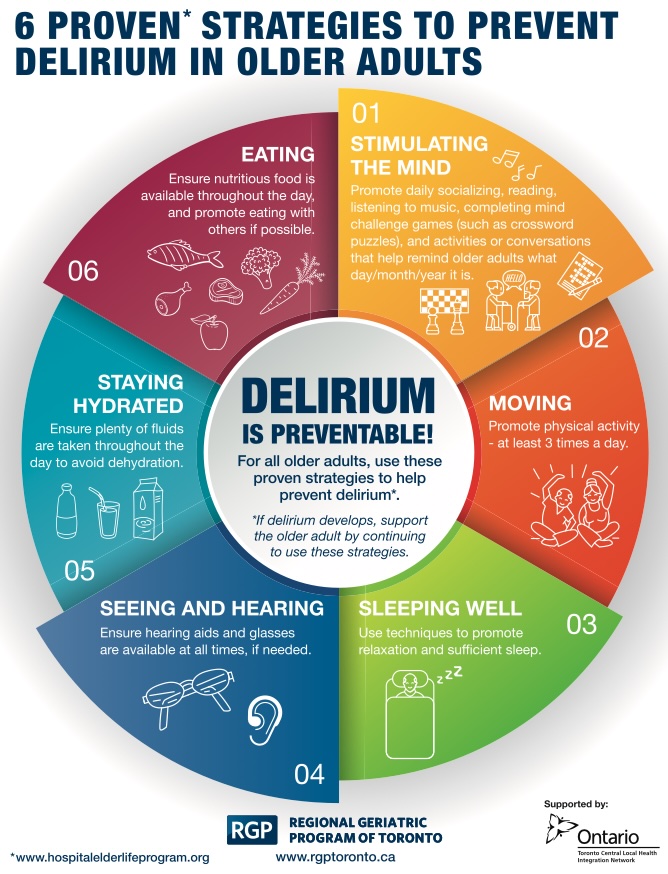
6 Proven Strategies to Prevent Delirium in Older Adults
This infographic highlights six evidence-based strategies that can help prevent delirium in older adults. It notes that if delirium develops, caregivers and healthcare providers should continue supporting these strategies.
- Stimulating the mind: Encourage daily socializing, reading, listening to music, completing brain-challenging activities such as crossword puzzles, and participating in conversations or activities that help maintain awareness of the day, date, and month.
- Moving: Promote physical activity at least three times per day, as appropriate for the individual.
- Sleeping well: Use techniques that promote relaxation and support sufficient, restorative sleep.
- Seeing and hearing: Ensure hearing aids, glasses, and other vision or hearing supports are available and used when needed.
- Staying hydrated: Encourage regular fluid intake throughout the day to help prevent dehydration.
- Eating: Ensure nutritious food is available throughout the day and encourage eating with others whenever possible.
Source: Hospital Elder Life Program and Regional Geriatric Program of Toronto.
Tell us what you think
Give us your feedback on this content by answering a few questions. Your participation will help us improve this resource. Take the survey.
_jpg.jpg?sfvrsn=bcb0dd6_2)